
Scars: The Overlooked Cause For Your Pain
Your scars shouldn’t be ignored:
In fact it can be why you haven’t gotten out of your pain and movement dysfunction.
Image of scar tissue and how it can impact many systems, including organs
Before we start, take a listen to the podcast episode that goes along with this blog! You can listen here, or on your favorite podcast streaming service. Just search for Uplift Wellness Pain Podcast and it will pop up! If you would rather watch on YouTube, Click HERE
How Scar Tissue Silently Drives Dysfunction, Sensitization, and Chronic Pain
Most people do not think about their scars. The surgery was years ago. The wound healed. Life moved on. But here is what nobody told you: healed does not mean resolved. A scar is not just a cosmetic reminder of something that happened. It is a permanent structural, neurological, and fascial change to your body, and it can be quietly driving dysfunction, compensation, and pain in ways that have nothing to do with where the scar actually is.
If you have been dealing with chronic pain that nobody can fully explain, if your rehab keeps plateauing, if your strength keeps coming back but the movement never quite feels right, your scar tissue may be a significant piece of the puzzle that has been overlooked.
This blog is going to walk you through exactly what scar tissue is, what it does to your body at a structural and neurological level, how it perpetuates pain and dysfunction, and what you can actually do about it, including things you can start doing at home today.
Part One: What Is a Scar? The Histology
To understand why scar tissue causes problems, you need to understand what it actually is at the cellular level. Scar tissue is not a perfect replacement for what was there before. It is a patch job, and the difference between the patch and the original has massive downstream consequences.
Your Skin Is Not Just a Covering
Before diving into scar formation, it is worth taking a moment to appreciate what skin actually is. Skin is the largest organ in the human body and one of its most sophisticated sensory systems. It is a direct gateway into both the peripheral and central nervous system, densely packed with mechanoreceptors, nociceptors, thermoreceptors, and proprioceptors that feed the brain a constant stream of information about the outside world and the body's relationship to it.
Developmentally, the skin and the nervous system share the same embryological origin, both deriving from the ectoderm, which means that from the earliest stages of human development, skin and brain are essentially the same tissue expressing itself differently. This is not a trivial detail. It means that anything disrupting the integrity of the skin, including a scar, is directly disrupting the input quality of one of the nervous system's most important sensory organs.
When tissue is damaged, whether through surgery, trauma, burns, or infection, heightened sympathetic drive is an immediate consequence. The nervous system interprets damage and tension in the skin as a threat and responds accordingly. This heightened sympathetic state drives vasoconstriction, which reduces local blood flow. It increases circulating stress hormones. It increases global muscular tone and shortens breathing patterns. The lymphatics constrict, creating stagnation, increasing local inflammation, and impairing the body's ability to clear waste products from the affected region. All of this, sustained over time, creates a compounding environment for pain and faulty movement.
The Four Phases of Wound Healing
Phase 1: Hemostasis (Minutes to Hours)
The moment tissue is damaged, the body triggers clotting to stop bleeding. Platelets aggregate and a fibrin clot forms as a temporary scaffold. Growth factors are released to signal the repair process to begin.
Phase 2: Inflammation (Days 1 to 4)
Immune cells flood the area. Neutrophils clear debris and bacteria. Macrophages arrive and orchestrate the repair process by releasing cytokines and growth factors. This phase is essential, but it becomes problematic when prolonged or dysregulated, which is extremely common in people dealing with chronic pain.
Phase 3: Proliferation (Days 4 to 21)
Fibroblasts migrate into the wound and begin laying down new collagen. This new collagen is predominantly Type III collagen, which is thinner, weaker, and significantly less organized than the Type I collagen found in healthy tissue. The wound fills in, but the new tissue lacks the structural integrity and organizational pattern of the original.
Phase 4: Remodeling (21 Days to 2 Years)
Type III collagen is gradually replaced by Type I. The tissue matures and strengthens. However, the collagen fibers in scar tissue never achieve the same organized, multi-directional basket weave pattern of healthy connective tissue. Instead, they are laid down in a parallel, unidirectional pattern that is significantly less capable of handling multi-directional forces. Research has confirmed that the remodeling phase can last up to two years, and that even mature scar tissue never fully replicates the organizational structure of the original tissue.
What Makes Scar Tissue Different
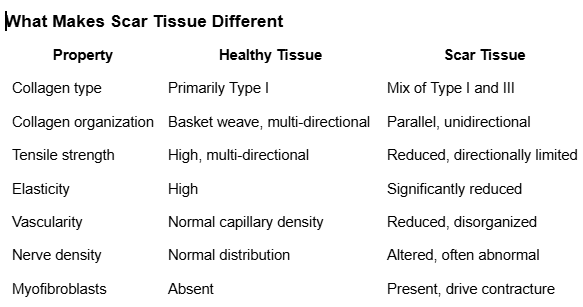
How scar tissue is different from normal healthy tissue
The presence of myofibroblasts is particularly significant. These are specialized contractile cells that actively pull wound edges together during healing. When their activity persists beyond the healing phase, they drive excessive scar contracture and restricted range of motion that compounds over time.
It is also worth distinguishing between hypertrophic scars, which are raised and remain within the wound boundaries, and keloids, which grow beyond the original wound margins. Keloids are associated with a higher density of sensory nerve fibers and mast cells, which may explain their pronounced tendency toward hypersensitivity and pain. Both types represent dysregulated healing responses that have significant implications for the nervous system and movement quality.
Part Two: Nothing Happens in a Vacuum — What Other Systems Are Affected?
A scar does not exist in isolation. It exists within an interconnected organism where every system communicates with every other system. When you understand how many systems a scar simultaneously affects, the idea that a scar from years ago could be contributing to your current pain stops being surprising and starts being obvious.
The Fascial System

Tom Meyer’s Anatomy Trains depicts how global the fascial system is, highlighting how one region can affect another via movement systems and fascial slings
Fascia is a continuous, three-dimensional web of connective tissue that surrounds and interpenetrates every muscle, bone, organ, nerve, and blood vessel in the body. It is not a passive wrapping. It is a dynamic, load-transmitting, mechanosensitive structure that plays a central role in movement coordination, proprioception, and force transmission across the entire body. Everything is connected through fascial connections and slings, and when there is a restriction or tension in one spot, there will be pulls distally that create tension, affect blood flow, alter sensory signaling, impact nerve flow and receptor stimulation, and change force distribution throughout the entire chain.
The fascial system also houses the interstitium, a fluid-filled space within the connective tissue that plays a critical role in waste clearance, nutrient delivery, and immune function. When tension and restriction are present in the fascia, fluid dynamics are impaired and the body's ability to clear waste products from the region decreases, contributing to local stagnation and inflammation.
The superficial fascia is particularly significant from a neurological standpoint. It is densely populated with mechanoreceptors that communicate directly with the deeper fascial layers and ultimately with the central nervous system. This means that working with the superficial fascia, whether through manual therapy, cupping, or taping, has the capacity to impact multiple layers of tissue all the way down to bone and joint.
The fascial system operates on the principle of tensegrity: compression elements such as bones and tension elements such as fascia, muscles, and tendons are balanced against each other to create a stable, adaptable structure. When tension is altered in one part of the system, it is transmitted throughout the entire network. Research has demonstrated that fascial layers in healthy tissue glide between 10 and 75 millimeters during movement and that connective tissue restrictions significantly reduce this gliding capacity. When that gliding is lost due to scar adhesions, the mechanical drag can be felt far from the original scar site.
Anatomy Trains and Distant Effects
The body's fascial continuities can be mapped into identifiable myofascial meridians, providing a clinical framework for understanding why a scar in one location can produce symptoms in a completely different region.
A C-section scar running horizontally across the lower abdomen sits directly in the path of the Superficial Front Line, which runs from the top of the foot through the anterior tibialis, rectus femoris, rectus abdominis, and sternocleidomastoid to the scalp. Restriction at the scar level can contribute to hip flexor tightness, altered lumbar mechanics, and even cervical dysfunction, with the client having no idea the two are connected.
A lateral knee scar from ACL reconstruction sits in the path of the Lateral Line, potentially contributing to hip abductor dysfunction, IT band tension, and altered cervical lateral flexion. An appendectomy scar in the lower right quadrant can create asymmetrical fascial tension that alters right hip mechanics, contributes to SI joint dysfunction, and changes load distribution through the lumbar spine. Research on epimuscular myofascial force transmission confirms that forces and restrictions travel between muscles through fascial connections, not within isolated structures.
The Circulatory and Lymphatic Systems
Initial tissue damage directly injures local blood and lymphatic vessels, altering the flow dynamics of the region immediately. But the downstream effects extend well beyond the acute injury phase. High tension in any one spot decreases the flow of fluid to and through that region, decreasing waste clearing, increasing stagnation, promoting inflammation, and contributing to swelling that feeds back into the pain cycle.
The vascular architecture within scar tissue is disorganized and less dense than healthy tissue. Research has confirmed that the vascular network formed within mature scar tissue is functionally inferior to the original. Reduced oxygen and nutrient delivery impairs the metabolic capacity of the tissue, reduces its ability to clear waste products, and contributes to a local environment that perpetuates low-grade inflammation and sensitization.
The lymphatic system, which drains interstitial fluid, immune cells, and waste products from tissues, is particularly vulnerable to fascial restriction. Even surgeries that do not directly involve lymph nodes can disrupt local lymphatic vessels within fascial layers. When lymphatic drainage is impaired by scar tissue, the normal resolution of the inflammatory process is disrupted, contributing to a state of chronic low-grade inflammation that directly sensitizes nociceptors. Research has further demonstrated that connective tissue plays a critical role in the movement of interstitial fluid and that restrictions in connective tissue mobility impair this fluid movement.
The Nervous System
The nervous system is where the scar story gets most complex. Scars affect the nervous system through multiple simultaneous pathways: mechanoreceptors, mechanosensitive nociceptors, literal nerve entrapment, and emotional encoding.
Scar tissue, by its very nature, applies tension to the surrounding system. Think of it like an internal stitch holding the tissue together. It creates tension to prevent further tearing. But that same tension transmits information continuously upward through the nervous system, altering sensation in the region and delivering nociceptive signals to the brain. When that nociceptive input reaches a sufficient quantity and frequency, the brain can output pain as a pathological reflex response, even in the absence of any new tissue damage.
During wound healing, nerve fibers regenerate into the scar tissue. This regeneration is frequently abnormal. Nerve endings become entrapped within the dense collagen matrix of the scar, creating a mechanical source of ongoing nociceptive input that is hypersensitive to mechanical stimulation. Even light pressure or normal daily movement can generate significant pain signals that feed directly into the central sensitization process. Research has confirmed that nerve entrapment in surgical scars and abnormal nerve regeneration within scar tissue are real, treatable, and frequently underdiagnosed sources of chronic pain.
Healthy skin and fascia are rich in mechanoreceptors including Meissner's corpuscles, Pacinian corpuscles, Ruffini endings, and free nerve endings. These structures provide the nervous system with constant information about touch, pressure, vibration, and movement. Scar tissue has a fundamentally altered mechanoreceptor profile, and the quality of sensory information being sent to the brain from that region is degraded. Research has quantifiably demonstrated altered pain and sensory thresholds in hypertrophic scar tissue.
This degraded sensory input has direct implications for movement quality. If the nervous system is receiving poor quality information from a region, it cannot produce precise, coordinated movement through that region. This is why post-surgical patients frequently show altered movement patterns even after tissue has healed and strength has been restored.
The brain maintains a somatosensory map of the body. When sensory input from a region is disrupted by scar tissue, the cortical representation of that region begins to degrade, a process called cortical smudging. Research has demonstrated extensive reorganization of primary somatosensory cortex in chronic pain patients, and cortical smudging is directly associated with increased pain sensitivity and reduced motor control precision.
As pain persists, the nervous system can become centrally sensitized, producing pain responses to stimuli that are not harmful at all. Central sensitization has been established as one of the primary mechanisms underlying chronic pain conditions of all types. Scars contribute to central sensitization through multiple simultaneous pathways: ongoing peripheral nociceptive input from entrapped nerves and ischemic tissue, degraded proprioceptive input that prevents accurate movement control, and the compensatory movement patterns the scar creates that overload other structures and generate additional nociceptive input.
Muscular Changes
When there is sufficient damage to muscle tissue, healing does not always occur through the original tissue type. Muscle tissue has two types of healing responses: parenchymal healing, in which the original muscle cells are restored, and stromal healing, in which fibrous scar tissue replaces the original muscle architecture. When stromal healing predominates, the result is a region of scar tissue within the muscle that has decreased contractile ability and fundamentally altered force transmission properties.
Muscle fibers have a specific directionality that is critical to their function. When scar tissue interrupts that directionality, it impairs the strength and function of the muscle and alters the distribution of force across it. This also impacts the brain's mapping of the region, because decreased proprioceptive information from the area reduces the precision of motor unit recruitment and movement control, especially when appropriate rehabilitation has not occurred. This can directly contribute to pain by decreasing function and driving compensatory movement patterns that overload surrounding structures.
Part Three: Scars and Emotional Storage
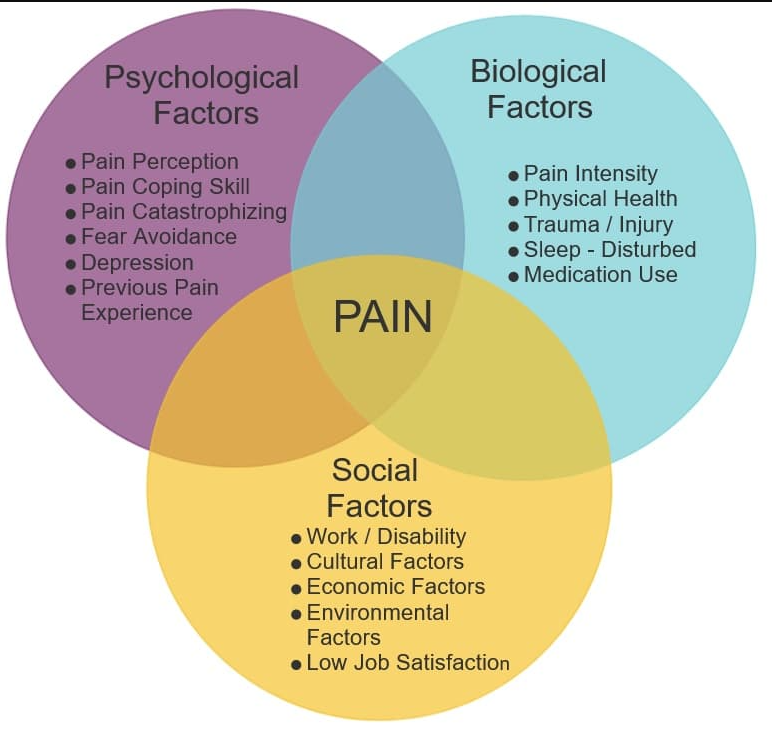
Biopsychosocial model of pain
This is the most frequently dismissed aspect of scar tissue management, and it is also the one that tends to produce the most powerful clinical responses when it is finally addressed.
The Science Behind Somatic Trauma
Every scar happens in the context of some form of trauma. One hundred percent of the time there is physical trauma. A significant portion of the time there is emotional trauma as well. At this point in the science, it is well established that emotions get stored as physical manifestations in the body. People commonly say things like "I carry my stress in my neck" or "when I get angry my back always tightens up." The same process occurs with scars.
The body creates associations between the emotional state present during the injury or surgery and the ongoing experience of having that scar, being limited by it, or simply living through the life circumstances surrounding that time period. Research has established the foundational science behind somatic trauma, demonstrating that traumatic experiences become encoded in the body and autonomic nervous system, producing physical symptoms including pain, tension, and altered sensation in the absence of ongoing tissue damage.
Polyvagal theory provides the mechanistic explanation: the autonomic nervous system, stuck in a sympathetically dominant state due to trauma, maintains a lower threshold for nociceptive signaling, keeps tissues in a state of chronic tension, and impairs healing and recovery.
Scars as Somatic Anchors
Consider this: if a scar is already delivering a steady stream of nociceptive information up to the brain, information that is already potentially pain-producing, and you add on top of that a negative emotional association, the brain will wire that emotion together with the scar and with pain. The nervous system is an association machine. It wires relationships together constantly.
If you are a coffee drinker who makes coffee every morning, when you wake up you will crave coffee and move toward the kitchen at the same time every single day, without consciously deciding to do so. Your brain wired all of the associations together, making it more likely to produce that habit as an automatic response to the morning context. The same process happens with emotions and scars.
In clinical practice, it is common to observe unexpected emotional responses during scar tissue work: sudden grief, anxiety, anger, or relief that the client did not anticipate and cannot immediately explain. These responses should be normalized and treated as clinically meaningful information. Research has documented the psychological impact of scarring and its effect on quality of life and pain perception, confirming that the emotional and physical dimensions of scar tissue are not separate systems.
A powerful clinical example of how deep this connection can go: a C-section scar over 30 years old, completely asymptomatic, was identified through NKT testing as a driver of a client's chronic back pain. When work was performed on that scar, an unexpected emotional release occurred, one the client did not know was still there. Her back pain, the emotional trauma surrounding a traumatic miscarriage, and the altered motor patterns that had developed in the years following were all linked, stored, and expressed together as a single interconnected pattern. Addressing the scar did not just change the physical presentation. It opened a door to an emotional resolution that had been waiting for decades.
Interoception and the Sensory Blind Spot
Interoception is the nervous system's ability to sense and interpret the internal state of the body. The insula integrates interoceptive signals and plays a central role in both body awareness and emotional processing. Scar tissue, by disrupting the quality of sensory input from a region, can create what clinicians describe as a sensory blind spot: a region of the body the nervous system has difficulty accurately perceiving, contributing to both physical dysfunction and a disconnected relationship with that part of the body.
Part Four: How Scars Create Movement Dysfunction and Perpetuate Pain
Local to Global: The Compensation Chain
Scars can cause both inhibition and facilitation of tissues both locally and globally. It typically starts as a local issue, and as that local issue develops over time, global movement patterns change to work around it. That ankle scar starts by affecting how the foot and ankle move. But as foot and ankle function degrades, the hip begins to adjust. The spine adjusts to the hip. The neck rotates to compensate for the spine. And suddenly there is a persistent pain in the neck that nobody can seem to fix, with no obvious connection to an ankle surgery that happened years ago.
Because the brain wires relationships together constantly, these compensatory patterns can become neurologically set, locked in as the default motor program. Add onto that the physical fascial distortions that mechanically change loading across the entire system, and you have a pattern that compounds and deepens over time without any new injury occurring.
Common clinical presentations that illustrate this perfectly:
A C-section scar restricts anterior pelvic mobility, drives the pelvis into posterior tilt, reduces lumbar lordosis, inhibits hip flexor function, and overloads the posterior chain, presenting as chronic low back pain, hip pain, or knee pain years after the surgery with no apparent connection to the original procedure.
A knee surgery scar from ACL reconstruction or meniscectomy creates local adhesions that restrict patellar mobility, alter quadriceps recruitment, and change force transmission through the knee, contributing to patellofemoral pain and altered gait mechanics that load the hip and lumbar spine differently.
An abdominal surgery scar of any kind can affect the function of the transversus abdominis and diaphragm by creating fascial restrictions that limit expansion and coordinated activation of these structures during breathing and movement, undermining the entire foundation of core stability.
A thoracic or mastectomy scar frequently inhibits the serratus anterior, producing the classic pattern of scapular dyskinesis, impingement syndrome, and cervical tension that is so common in post-surgical thoracic patients.
Visceral Scars and the Gut-Brain Axis
Surgical scars involving the abdomen can affect visceral fascia and create adhesions around the organs themselves. Research has shown that abdominal adhesions are present in up to 90 percent of patients who have had previous abdominal surgery and are a leading cause of chronic abdominal pain, digestive dysfunction, and referred pain patterns. The enteric nervous system, the gut's own extensive neural network, means that visceral nociception from adhesions can contribute to central sensitization through the gut-brain axis, creating a pain perpetuation pathway that is entirely disconnected from the original surgical site.
The Overlapping Pain Perpetuation Mechanisms
Ongoing nociceptive input from the scar drives central sensitization. Central sensitization drives fear avoidance of movement. Fear avoidance reduces tissue tolerance. Reduced tissue tolerance reinforces dysfunctional movement. Dysfunctional movement perpetuates sensitization. And the scar driving all of it may not even be painful to the touch.
Layered on top are the additional contributors that make chronic pain so complex: emotional trauma, financial stress from lost work capacity, the psychological damage of being dismissed by clinicians, and systemic inflammation from poor sleep and nutrition. This is not a simple problem and it does not respond to simple or generic treatment.
Part Five: Neurokinetic Therapy and Scar-Driven Inhibition
What Is NKT?
Neurokinetic Therapy (NKT) is an assessment and treatment system grounded in motor control theory. It operates on the understanding that the motor control center, a functional region of the cerebellum, stores and coordinates movement programs that dictate how muscles are recruited during any given task. When the system is disrupted by injury, scar tissue, or pain, the motor control center compensates by finding alternative recruitment strategies that become stored as new programs, making the dysfunction self-perpetuating.
The assessment uses manual muscle testing as a biofeedback tool to identify which muscles are neurologically inhibited (underactive) and which are facilitating (overactive and compensating for the inhibited ones).
How Scars Create Motor Control Dysfunction
In NKT terminology, a scar becomes a facilitated structure: something the nervous system is constantly monitoring and bracing around. The muscles that have adapted to protect the scar become neurologically overdriven. The muscles that should be doing the primary work become inhibited and test weak on manual muscle testing.
The critical clinical insight is this: the scar does not have to be painful to be driving this pattern. A completely asymptomatic surgical scar from years ago can be actively inhibiting muscle function and producing pain somewhere entirely different in the body.
The NKT Assessment Protocol for Scars
Step 1: Identify the inhibited muscle. The practitioner tests a muscle relevant to the client's pain pattern or movement dysfunction. A weak test indicates neurological inhibition rather than true weakness.
Step 2: Confirm the scar as the facilitating structure. Light contact is placed on the suspected scar while retesting the previously inhibited muscle. If the muscle now tests strong, the scar is confirmed as the driver of the inhibition.
Step 3: Release the facilitated scar. The practitioner treats the scar using appropriate manual therapy techniques while the client performs an activation exercise for the previously inhibited muscle. This dual input is designed to update the motor control center's stored program.
Step 4: Retest and assign homework. The previously inhibited muscle is retested to confirm the neurological change. The client is given a specific home program involving release of the scar followed immediately by activation of the previously inhibited muscle. This homework is critical because the motor control center will revert to the old program within 24 to 48 hours without consistent reinforcement.
Why NKT Works Where Strengthening Alone Does Not
If a muscle is neurologically inhibited by a facilitated scar, no amount of strengthening exercise will fully restore its function. You can perform hundreds of repetitions targeting that muscle, but if the motor control center is actively suppressing its recruitment in favor of a compensation pattern, the exercise will either be performed by the compensating muscles, or any improvement will be temporary and will quickly regress.
This explains why so many people do their physical therapy exercises diligently and plateau or regress. The exercises may be entirely appropriate. The problem is that the root cause driving the inhibition has never been identified or addressed. Until the motor control center receives a new input that updates its stored program, the old pattern will persist.
A few clinical examples that illustrate just how specific and powerful this approach can be:
A C-section scar facilitating the rectus abdominis and inhibiting the transversus abdominis. Research has established a direct relationship between transversus abdominis inhibition and lumbar instability. When the TvA is inhibited by scar facilitation, the entire foundation of core stability is compromised, and no exercise program will fully restore it until the scar is addressed.
A knee surgery scar inhibiting the VMO. Research has demonstrated delayed onset of VMO recruitment relative to the vastus lateralis in patellofemoral pain syndrome. When the VMO is inhibited by scar facilitation, the patella tracks laterally, loading the lateral facet and producing anterior knee pain that is frequently mismanaged as a strength problem.
A thoracic scar inhibiting the serratus anterior. Research has confirmed the clinical significance of serratus anterior inhibition in shoulder dysfunction and the downstream effects that follow when scapular stabilization is lost.
An appendectomy scar inhibiting the right psoas. The psoas is both a primary hip flexor and a critical lumbar stabilizer. When inhibited, the lumbar spine loses segmental stability, the SI joint is stressed asymmetrically, and the TFL overworks as a compensatory hip flexor, contributing to IT band tension and lateral hip pain that has no obvious connection to the original surgery.
Part Six: What You Can Actually Do About It
Working With a Professional
The most comprehensive scar management happens with a trained practitioner who can assess the full scope of the scar's influence: fascial restrictions, motor control inhibition, nervous system sensitization, and emotional components. If you are dealing with chronic pain and you have any surgical or significant traumatic scars in your history, that history needs to be part of your assessment. Ask your provider specifically whether they assess and treat scar tissue, and whether they have training in approaches such as NKT, myofascial release, or visceral manipulation.
At-Home Treatment Options
While professional treatment is the most comprehensive approach, there is a significant amount you can do at home to begin addressing your scar tissue between sessions or as a starting point before pursuing professional care. Consistency matters more than intensity here. Gentle, regular input is more effective than aggressive occasional work.
1. Manual Scar Tissue Mobilization
Direct manual therapy applied to scar tissue is the foundation of scar management. Research has found evidence for improvements in scar pliability, pain, and tissue quality through regular massage and mobilization work. You do not need a professional to perform basic scar mobilization at home.
How to do it:
Wait until the wound is fully closed and the tissue is no longer fragile, which is typically 6 to 8 weeks post-injury or surgery for most superficial scars. Always get clearance from your surgeon or healthcare provider before beginning scar massage.
Start by placing two or three fingers flat on the scar with light but firm pressure. Without sliding across the skin, sink into the tissue and begin moving in small circles, moving slowly in all directions: up, down, left, right, diagonal. You are looking for directions that feel restricted, stuck, or tender. When you find one, hold gentle sustained pressure in that direction until you feel the tissue begin to release or soften, which typically takes 30 to 90 seconds. Then move to another direction.
Progress over time to deeper pressure and to mobilizing the tissue by picking it up between your fingers and gently rolling it, which addresses the deeper fascial adhesions between layers. Work not just on the scar itself but in the surrounding tissue, which is often where the fascial restriction extends.
Duration: 3 to 5 minutes per session, once or twice daily.
What to expect: Mild discomfort and sensitivity is normal, especially early on. Sharp or severe pain is not. You may notice temporary redness and increased sensitivity after a session, which is a normal response to increased circulation.
2. Cupping
Cupping creates a negative pressure that lifts and separates fascial layers that have become adhered. Unlike compression-based manual therapy, the decompressive force of cupping specifically targets the superficial and intermediate fascial adhesions that restrict gliding. Research has demonstrated both pain reduction and tissue mobility improvements with cupping applied to myofascial restrictions.
Silicone cupping sets are affordable, widely available, and safe for home use when applied correctly.
How to do it:
Apply a thin layer of body oil or lotion to the skin around the scar to allow the cup to glide. Squeeze the silicone cup, place it on the skin adjacent to or directly over the scar, and release. The cup should create a gentle suction that visibly lifts the skin. Do not use a suction strong enough to cause significant bruising or pain.
You can use the cup in two ways. Static cupping involves leaving the cup in place for 2 to 3 minutes and letting the sustained decompressive force work on the tissue underneath. Gliding cupping involves gently moving the cup across the skin in slow strokes along the length of the scar and into the surrounding tissue, which addresses a broader area of fascial restriction. Both approaches are beneficial.
Work not just directly on the scar but in the surrounding region, because the area of fascial restriction typically extends well beyond the visible boundaries of the scar.
Duration: 5 to 10 minutes per session, two to
3. K-Tape
When K-tape is applied correctly over scar tissue, the elastic recoil of the tape creates a continuous, gentle lifting effect on the skin. That lift decompresses the tissue underneath it, and that decompression does several things simultaneously. It improves local circulation by reducing the compressive tension that scar tissue places on the surrounding blood vessels, allowing more oxygen and nutrient delivery to a region that is often chronically underserved.
It supports lymphatic drainage by creating a slight negative pressure that encourages lymphatic fluid to move through channels that have been compressed or restricted by the scar and surrounding fascial adhesions. It also changes the lines of tension acting on the scar and surrounding tissue, which can produce an immediate reduction in discomfort and an improvement in local mobility that surprises most people the first time they try it.
How to do it:
The single most important thing to understand about applying K-tape to a scar is this: zero tension on the tape itself. This is where most people get it wrong. K-tape does not work by pulling the tissue into a different position. It works by laying on the skin with no stretch, so that the tape's natural elastic recoil creates the lift. If you stretch the tape before applying it, you lose the decompressive effect and replace it with compression, which is the opposite of what you want.
Basic application:
Make sure the skin is clean, dry, and free of lotion or oil before applying
Cut a strip of K-tape long enough to cover the scar and extend an inch or two beyond each end
Tear the backing paper in the middle of the strip, not at the ends
Hold the tape by the backing paper, lay the middle of the strip directly over the scar with zero stretch, and smooth it down
Peel the backing off the ends last, laying those anchor points down with absolutely no tension
Rub the tape firmly to activate the adhesive with the heat of friction
For broader fascial restriction, apply a second strip perpendicular to the first, creating an X or cross pattern over the scar. This addresses restriction in multiple directions simultaneously.
Duration: It can stay on for up to 3 days (depending on the quality of the tape). Take it off at 2-3 days and don’t re-apply for another day or so.
A few practical notes:
K-tape is water resistant and can be worn in the shower
If you notice significant skin irritation, remove it immediately and allow the skin to recover before reapplying
Apply to fully healed skin only, never to open wounds or fragile healing tissue
Always get clearance from your surgeon or healthcare provider before beginning any scar treatment, including taping
Your Scar Has Been Telling Your Body a Story. It's Time to Change the Narrative.
If you have made it this far, something in this blog probably resonated with you. Maybe you have a scar you never thought twice about. Maybe you have been dealing with pain that nobody can fully explain. Maybe you have done the exercises, tried the treatments, and keep hitting the same wall.
Here is what we want you to know: it is not you. It is what has not been assessed yet.
Scar tissue is one of the most consistently overlooked drivers of chronic pain and movement dysfunction in clinical practice. It does not show up on most imaging. It rarely gets asked about in a standard intake. And yet it can be quietly running compensation patterns, inhibiting muscles, sensitizing your nervous system, and perpetuating pain for years, sometimes decades, after the original injury or surgery.
The good news is that when you identify it, assess it properly, and treat it as part of a comprehensive plan, things change. Sometimes dramatically. Sometimes in ways that surprise everyone involved.
Ready to Find Out If Your Scar Is Part of Your Pain Story?
At Uplift Wellness in Kingston, NY, every evaluation starts with the whole picture. Your scar history. Your movement patterns. Your nervous system's current state. The actual drivers of what you are experiencing, not just the symptoms sitting on top of them.
We work with people who have tried other things and hit walls. People who have been told their imaging looks fine but still hurt every single day. People who are tired of being handed a generic program that does not account for any of the things we talked about in this blog.
If that is you, the best place to start is a free intro call.
On that call we will:
Hear exactly what you are dealing with and how long it has been going on
Walk you through how we work and whether it is the right fit for your specific situation
Book you for your eval so we can get you on the best path moving forward
We do not make claims about whether we can help you until we actually spend time with you and do a thorough assessment. Because that is the only honest way to do this work.
Your Exclusive Offer
As a reader of this blog, you get $100 off our 90-Minute Deep Dive Evaluation when you book your intro call.
This is our most comprehensive assessment, specifically designed to identify every contributing factor to your pain, including scar tissue, motor control inhibition, fascial restrictions, nervous system sensitization, and movement dysfunction. It is where the real work begins.
📧 info@upliftwellness.org
📲 845-303-2976
📍 Kingston, NY
"If you've tried every therapy or program and nothing's worked… it's not you. It's the program."
Your scar has been part of your story long enough. Let's find out what it has been doing, address it properly, and start writing a different one.
Stop Guessing. Start Progressing.
— Mike Carroll, LMT | Owner, Uplift Wellness

About the Author
Mike is a Licensed Massage Therapist, movement specialist, and strength coach serving the Hudson Valley. He helps clients move beyond pain through personalized, root-cause-focused care combining manual therapy, NKT, and strength training.
Serving Kingston, Saugerties, Rhinebeck, Red Hook, Woodstock, Catskill & Poughkeepsie in the Hudson Valley.
Stay Connected. Keep Progressing.
Get expert tips on movement, strength, recovery, and pain relief straight to your inbox.
Short, practical insights designed to help you feel better between sessions.
⬇︎ Sign Up for the Newsletter below